HEALTHCARE QUALITY PAGE

BLOG APRIL 2025
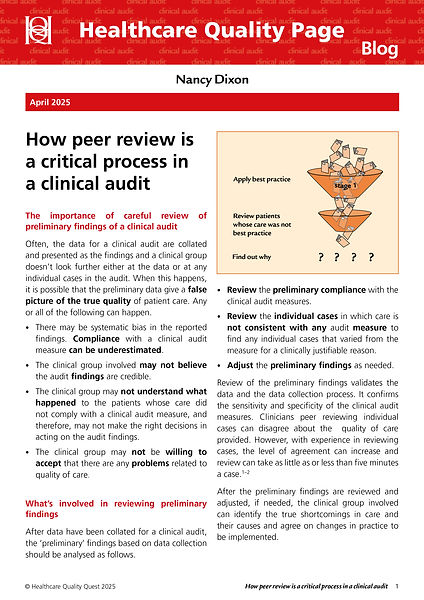
How peer review is a critical process in a clinical audit
Clinical audit findings from data collection are often accepted as the true picture of patient care without further peer review. The data are collected, the findings are presented, and the group moves on to deciding if anything needs to be done about the audit findings. But there is risk in not looking further at the data. If the group doesn’t look at what happened to the patients whose care appeared not to meet the audit measures, the data can give an incomplete — or even misleading — story about the true quality of care.
The second stage look matters because several things can go wrong when audit data are accepted without peer review:
-
There may be systematic bias in the reported data because compliance with good practice is underestimated.
-
Clinicians may not trust the findings or see them as credible.
-
The group may not understand what actually happened for patients whose care did not match the audit measures.
-
The group may resist accepting that there are quality-of-care problems to address.
-
The wrong decisions may be made about what action, if any, should follow the preliminary findings.
Peer review helps turn preliminary audit findings into a more clinically meaningful picture. It gives the clinical group a structured opportunity to identify legitimate exceptions to the measures — for example, an exception that was forgotten, an extremely rare case, a complex case involving multimorbidity, or a state-of-the-art exception where the evidence is uncertain or conflicting. In other words, peer review is not a defensive exercise. It is a way of making sure that audit findings are fair, credible, and sufficiently valid to guide improvement.